We all suffer from common cold, and that, frequently. Why have we not developed immunity against it till now? By immunity I mean immunity as a species.
$\begingroup$
 $\endgroup$
$\endgroup$
2
asked Sep 21, 2014 at 5:24
-
2$\begingroup$ The short answer is we do, it's just that there are so many different causes to common cold. A slightly longer and more complete answer will note that while we know immunodominate epitopes for the 100s of rhinovirus serotypes, we are still researching why viruses like RSV are not immunogenic (my bet is on NS1, possibly NS2 proteins). If no one has put up a good answer by 2100ish EST, I should be back on then to post one. $\endgroup$– Atl LEDCommented Sep 21, 2014 at 7:06
-
$\begingroup$ What kind of immunity are you talking about? Immunity as a species? Immunizations? Can you clarify? $\endgroup$– anongoodnurseCommented Sep 21, 2014 at 8:22
Add a comment
|
2 Answers
$\begingroup$
$\endgroup$
7
Long lasting immunity is obtained by means of the adaptive immune system, and mainly involves the development of antibodies that identify specific parts (epitopes) of the pathogen's proteins. Common cold is typically caused by a type of virus called rhinovirus. Viruses have very high mutation rates, which alter the sequence of the virus proteins, modifying their antigenic properties. This consequently alters the ability of antibodies to recognize a particular antigen.
In other words, we do develop long lasting immunity against the virus that causes us a cold today, but the virus that causes us a cold a few months later is somewhat different, and the adaptive immune system has to start from scratch.
-
1$\begingroup$ Why do viruses have high mutation rates? Because thay divide so fast? $\endgroup$ Commented Sep 21, 2014 at 13:44
-
6$\begingroup$ @kinshukkashyap it is because the higher error rate in the genome replicating enzymes. For example, retroviruses use reverse transcriptase that has high error rates (due to lack of proofreading). $\endgroup$– ddiezCommented Sep 21, 2014 at 14:13
-
$\begingroup$ @kinshukkashyap, but, it is also connected to faster replication times. If you divide very fast and can produce a large amounts of copies (offspring) then you can accept higher replication errors that may render some of the copies useless, but may lead to some advantage to some other copies (e.g. drug resistance). $\endgroup$– ddiezCommented Sep 21, 2014 at 14:16
-
$\begingroup$ @ddiez I'm not sure if mutation rates are the most important factor here, as forward genetic experiments with HRV don't show the virus changing serotypes often. $\endgroup$– Atl LEDCommented Oct 1, 2014 at 18:46
-
$\begingroup$ @AtlLED, could you provide reference for that experiment? Indeed, there are several mechanisms for immune evasion. Serotype changing is one of them. In viruses there is also antigenic drift (caused by mutations) and shift (caused by exchange of sequences between viral strains), Ref Janeway's Immunobiology 5th edition. It has been postulated that HRV uses antigenic drif/shift but cannot find references demonstrating that! $\endgroup$– ddiezCommented Oct 2, 2014 at 4:28
$\begingroup$
$\endgroup$
1
First, I want to note that ddiez has a good answer, but I thought this was good question to have a more expanded answer on immunology and pathogenesis.
The First thing we need to establish what is a "cold".
The most common cold is rhinovirus (HRV), but the second place holder is a little harder to define. For example, respiratory syncytial virus (RSV) has been shown to be nearly ubiquitous by age two. I actually disagree with the Wiki article on the common cold which puts coronaviruses (plural, which is not clear in the article) in second place. For example, if you take look at sessional reports from hospitals, you can find that RSV and influenza are the more common. Now this does select for those who were sick enough to seek hospital treatment, but if you look at a recent more in-depth study conducted through health clinics, you will again find coronavirus in much lower showing:
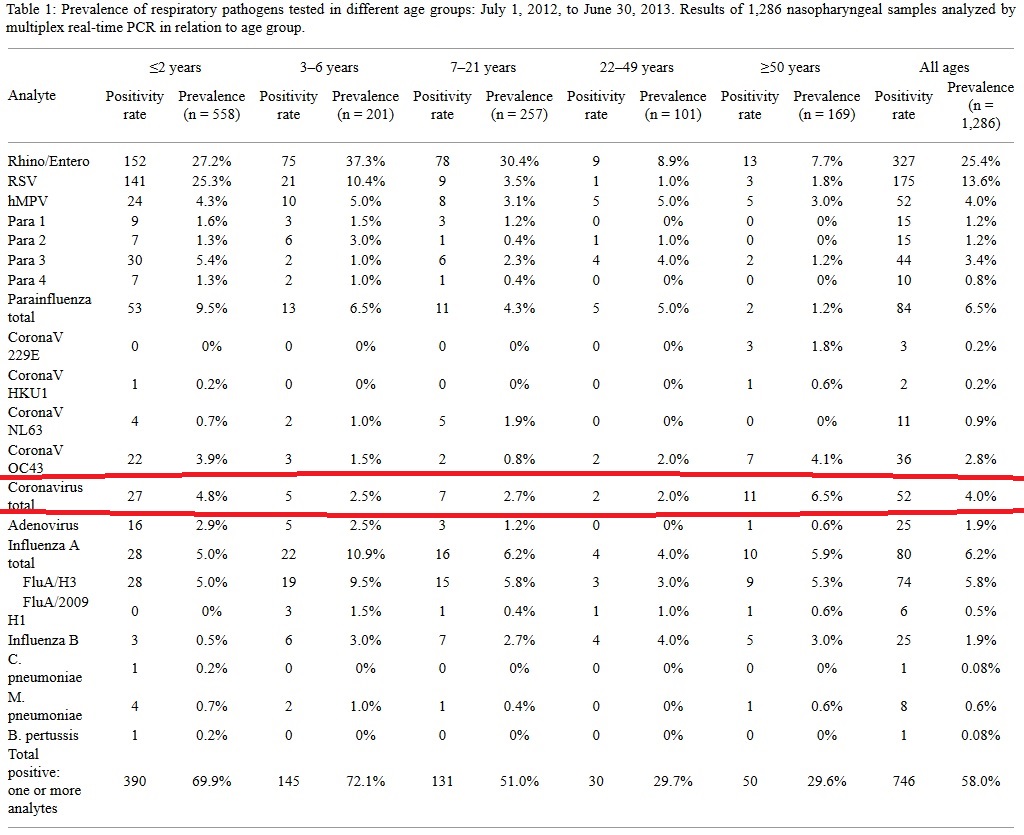
[Editorial note, if someone wants to take the time to MathJax that table in, please go ahead. It seemed too large to insert the table as text. Here’s the original.]
Thus, a cold is an infection from any of the above viruses, with a common cold likely being HRV or RSV. But how the body reacts to each of those is different.
Secondly, how do we mount an immune response to a cold?
There are two different kinds of immune responses in humans: innate or adaptive (to not get to technical, you can come up with responses outside of these). Both responses are excitingly complex, and needed to fight a cold. The innate immune system is designed to handle the initial reactions to the pathogens, but often the adaptive immune system is what "clears" (viral clearance being the removal of the infection) the infection totally. In a novel infection, the adaptive immune system takes a few days to ramp up, which is why a cold can last for a few days to two weeks. This is when you get B-cells producing enough antibody to clear the infection. Then the next time you are infected by something of the same serotype you will have a reservoir of cells already primed to make an immune response, and it will happen quicker. At least that is what the human body is trying to do. Viruses are trying to "evade" the immune system and proliferate (acknowledging of course that is a personification of viruses, and that they are not "trying" to do anything).
The key word in the adaptive response is "novel." If the pathogen is different enough, that is the epitopes are different enough, then the immune system won't recognize it. This is the principal strategy used by HRV. Depending on who you ask there are between 96-120 serotypes of HRV, so using a number of about 100 seems reasonable (120 is a much more recent number and the increase has largely correlated with better diagnostic tools). There don't seem to be additional stereotypes developing/mutating quickly (though conceivably they could), so as opposed to being infected by a mutated version of the cold you had last year, you're getting a different strain/serotype that was already in circulation. Thus if you got a different HRV infection once a year, you have about 100 years of rihno viruses colds (when you actually get that old you have senescence problems in the immune system).
RSV is a different story. You don't mount a lasting immune response to the virus in the first place:
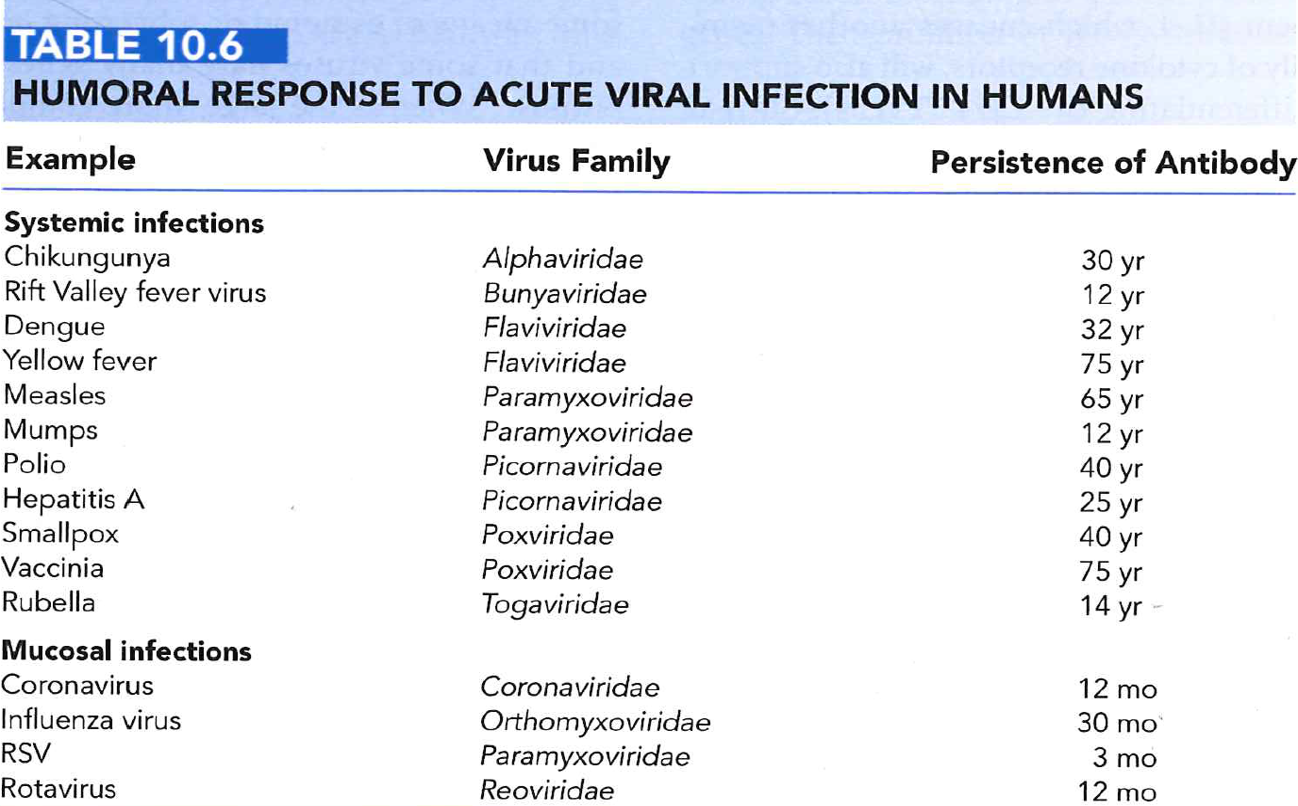 (Table 10.6. Fields Virology; 6th Edition. LWW 2013)
(Table 10.6. Fields Virology; 6th Edition. LWW 2013)
In fact, I know a researcher who would infect his lab members with the exact same strain of RSV every 6 months for years (before people would stop such a thing...). Why RSV doesn't elicit lasting immunity--and in fact notably shorter immunity--is the subject of current research.
As you can see in Table 10.6, mucsal responses are generally not as long lasting as systemic infections. This can make sense from a macro view—the mucus successfully prevented the pathogen from spreading to the rest of the tissues in the body, so it's not as critical to respond to. On a more specific level we know that more IgA is produced and the cytokines can be different. But RSV seems specifically reduced. One leading idea is that two of the proteins produced by the virus, NS1 and NS2, cause an immune response to not be properly mounted. In other words, the virus is making materials that deliberately interfere with adaptive immune response. An interesting paper that just came out addresses this idea for a possible vaccine candidate.
-
1$\begingroup$ This should be the accepted answer. $\endgroup$ Commented Aug 19, 2019 at 16:16