Cornelius covers Primary Infection and some of Dissemination.
Wysiwyg covers some reasons when HIV cannot proceeds to AIDS.
Little however is discussed yet exactly about the Pathogenesis - how HIV proceeds into AIDS.
There are many stages:
- Primary infection
- Dissemination of virus to lymphoid organs
- Latency
- Increased HIV expression
- Constitutional symptoms
- AIDS
- opportunistic diseases (etc pneumocystis pneumonia - P. jirovecii for human; HIV-induced thrombocytopenia; ...)
- death
Cornelius nicely mentions that HIV infects CD4+ T lymphocytes, macrophages and dendritic cells.
In other words, HIV infects CD4+ T lymphocytes and the major Antigen Presenting Cells (APC).
Also monocytes are infected.
These infected cells play a major role in dissemination and pathogenesis of HIV infection.
Antigen presentation couples innate and adaptive immune system.
Any attack on those cells will be difficult to control:
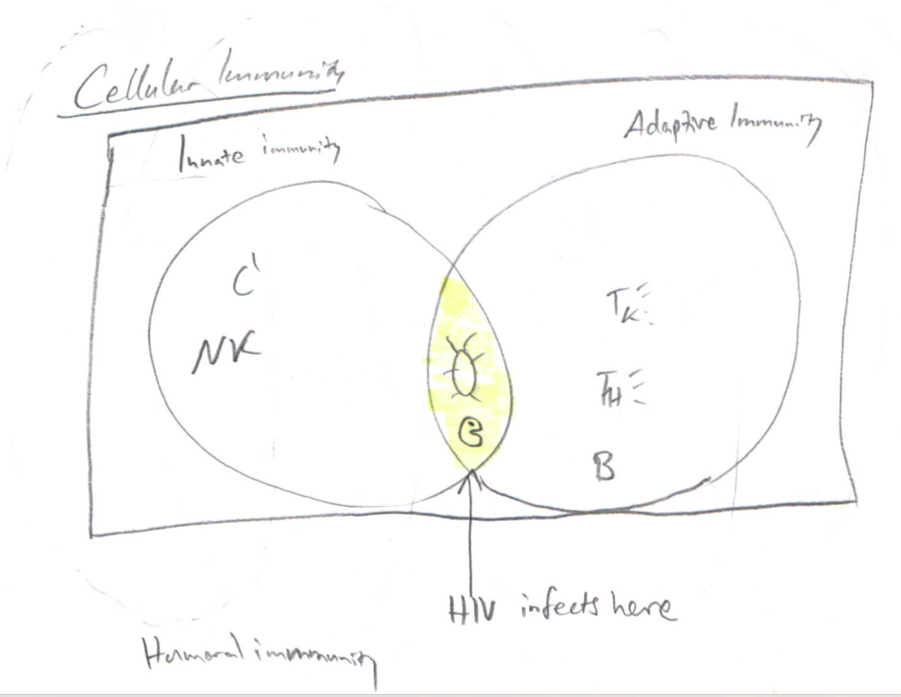
where I left NK cells only to innate immunity because they do not participate in antigen presentation.
Innate and adaptive immune systems are visualised on the plane.
You have then humoral immunity working around that plane as circles.
I emphasize with that the local nature of humoral immune system and how it extends the cell-mediated immune system.
Any attack on the heart of this system i.e. antigen presentation will also risk the humoral immunity and thus cause fast progression of the disease.
These APCs act as reservoirs for HIV virus in the body during latent period and after the latent period.
However, there is very active replication of the virus also during the latent period in these reservoirs.
The virus replicates actively in lymphatic system.
This is why you see steady level of HIV virus in blood during first eight years, see Figure below [Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology, 7e > Section 27. Viral Diseases of Skin and Mucosa].
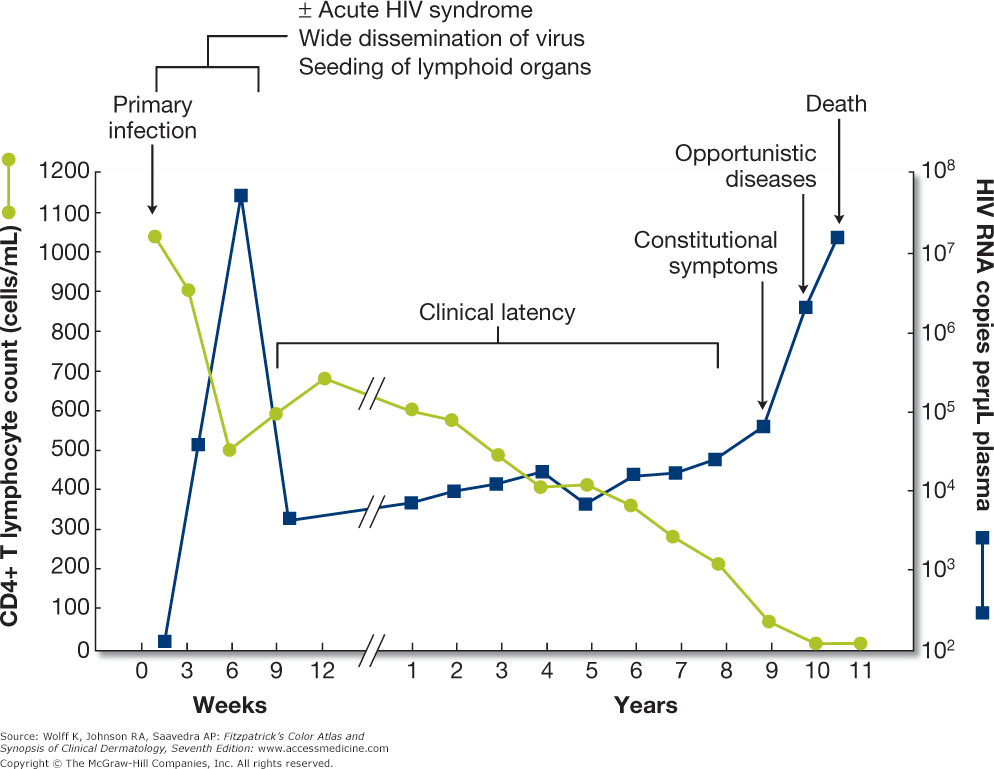
The structure of lymph nodes is disrupted eventually.
There is a degeneration and loss of virus holding function.
Virus leaks into the blood which can be seen as increased viral load at about 7-8 years after infection when constitutional symptoms start.
This amount of virus is very large that is released into circulation.
There is a rise in viremia.
Now the infection becomes T-tropic (proliferates and replicates actively on CD4+ T lymphocytes), while it was M-tropic (proliferates and replicates actively on APCs in lymphatic circulation) until the start of AIDS.
Actually, these APCs play a major role in trapping the virus, until their architecture changes.
Some antiviral drugs work on these CD4+ cells i.e. at least macrophages coupled with MHC II complexes.
There is still much unknown in the pathogenesis of HIV:
- role of dendritic cells in M-tropic phase
- role of dendritic cells in T-tropic phase and restricting the functioning of HAART (Highly Active Antiretroviral Therapy) therapy.
and there exist no antiretroviral drug which can target the major antigen presenting cells or use another way - to stop viral replication completely.
Cornelius writes HIV virus kills CD4+ cells.
It is better to say HIV virus decreases CD4+ cell count.
Killing is just one mechanism.
The mechanisms are
- HIV can induce apoptosis of CD4+ cells
- lysis of CD4+ cells
- killing (natural killers, macrophages)
- networks (CD4+ cells will bind to other CD4+ cells so cells cannot work)
- gp120 antigenic - which attach to CD4+ antibodies
which decreases CD4+ cell count.
Sources
- Thomas, C. F, et al. Pneumocystis Pneumonia. The New England Journal of Medicine. 2004.
- Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology, 7e > Section 27. Viral Diseases of Skin and Mucosa.
- My class notes 2014-2016.