Suppose you want to convert the skin cell into a pluripotent stem cell. I know there are a few genes that were identified for this purpose (a recent Nobel Prize). But apart from finding such genes, it also seems to involve maintaining the right environment, such that some critical receptor doesn't get triggered and alter the entire expression. It also seem to involve ensuring gene expression stability after the change has occurred. Could someone add to this? What are the broad paradigm ideas in stem cell engineering?
Add a comment
|
2 Answers
$\begingroup$
$\endgroup$
Current reprogramming technology, pioneered by Takahashi and Yamanaka 1, was built on several seminal advances in the field of developmental biology. First, nuclear transfer experiments demonstrated that a somatic cell nucleus could be epigenetically reset to an early developmental state [2]. Second, cell culture conditions were developed that allowed for the isolation and culture of pluripotent cells, termed embryonic stem (ES) cells, from the inner cell mass of the human and mouse blastocyst [3,4]. Finally, study of these cells and of early embryonic development led to the identification of factors that were ultimately able to reprogram mouse embryonic fibroblasts (MEFs) to the iPS cell state when ectopically expressed, albeit at low frequency.
Reprogramming of somatic cells is a multistep process that culminates in the expression of pluripotency genes such as Nanog. Although morphological changes occur at early and intermediate stages of reprogramming, pluripotency gene expression is only induced during the late stage and indicates faithful reprogramming.
The core reprogramming cocktail, consisting of the transcription factors Oct4, Sox2 and Klf4 can be augmented by the addition of factors that enhance the efficiency of iPS cell generation
Its a multistep process in which much research is still needed,
The frequency with which somatic cells convert to iPS cells is typically below 1%. Therefore, much effort has gone into improving reprogramming.
specially to increase efficiency of iPS cell generation
The ability of cells to pass through the cell cycle has also been shown to be an important determinant of reprogramming efficiency. Knockdown or gene deletion of p53, p21 or proteins expressed from the Ink4/Arf locus allows cells undergoing reprogramming to avoid the activation of cell cycle checkpoints and cellular senescence, leading to greater iPS cell formation [21],24-27].
$\begingroup$
$\endgroup$
First and foremost, stem cell therapies are cell therapies that, in the US, are regulated by such agencies as FACT (foundation for the accreditation cell therapies), CAP (college of American pathologists) and the FDA (food & drug administration). Manufacturing must be compliant under GTP (good tissue practice) and GMP (good manufacturing practice) standards. Even the labeling of products is moving to the harmonized system ISBT128, managed by ICCBBA (International Council for Commonality in Blood Banking Automation). The take-home point here is that everything is tightly regulated, and produced under rigorous standards of safety, conformity and documentation. Not everyone is FACT accredited, but the benefits are becoming of increasing importance, especially to insurance providers (ref). The therapies are costly to manufacture, to be certain. The two FDA-approved CAR-T immunotherapies YESCARTA and Kymriah run around $500,000.
So you have a number of types of stem cell therapy. Bone marrow transplantation is considered a stem cell therapy, and then you have therapies that involve human embryonic stem cells (hESC) and human induced pluripotent stem cells (hiPSC).
In terms of hiPSC, groups have been successful both in culturing with transcription factors such as Oct4, Sox2, Klf2 and so forth, and in using sendai virus to deliver these transcription factors directly within the cell (thermofisher's Cytotune®-iPS Sendai Reprogramming Kit, youtube video).
We can also see, however, that stem cells can be obtained elsewhere and don't necessarily need to be induced. You can source hESC from embryos and cord blood, and hematopoietic stem cells (HSC) can be mobilized from the marrow with a drug cocktail (like plerixafor and GM-CSF) and harvested with apheresis.
So just for a real-world example of what you're thinking: Papers on the production of glucose sensitive insulin-secreting ß cells from hESC using carefully controlled culture conditions have been published (ref), and companies have taken advantage of this technology. Subdural implants using this system are in clinical trials right now. They produce the ß cells from hESC by controlling the cultures:
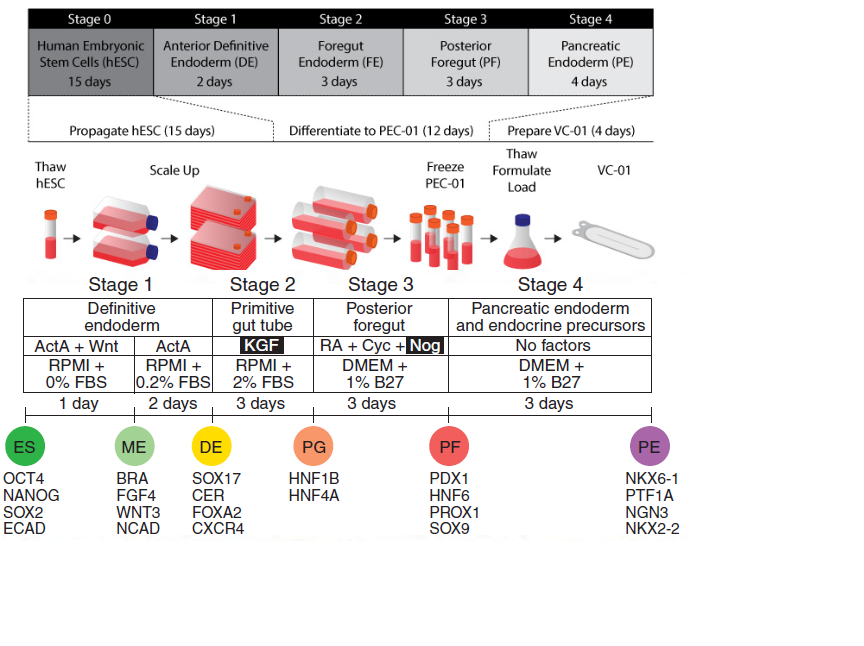
The transcription factors along the bottom of the figure, which I've pasted together from two sources, shows what transcription factors should be active at that stage. The identity of the final product can be surmised from a combination of what transcription factors should and should not be active. It's also important to realize that there will be off-target cells, but that the process should be validated to ensure on-target cells stay within an acceptable range as defined during pre-clinical development.
Manufacturers would also need to test for the purity, sterility, endotoxin and potency of their cells. Potency assays have become something of a prerogative for the FDA, since anyone can produce a cell, but how can they say it's effective or does what it's marketed to do? An example potency assay might be two cultures, one with glucose and one without, does one secrete more insulin than the other? You'd pick this assay because the proposed mechanism of action for ß cells is they respond to glucose, and secrete insulin.
For sterility, they sell some good kits like BacT alert aerobic and anaerobic test bottles, mycoplasma testing kits, you can also do culture plates and gram stain. Products that don't exhibit 100% sterility can't be infused, and so it generally follows that exceptional releases can be made for many other issues by a physician, but contamination will stop a cell therapy product dead in its tracks.
You're also right in that cell therapies which involve a gene modification step need to look at such things as transduction efficiency, live virus titer, expression of molecules related to the transduction and so forth. The sendovirus kit referenced above is a fair pick because as they demonstrate, after several passages the non-integrating virus titer is negligible. For human administration, in the CAR-T space, the FDA has required that studies where CAR-T have been infused follow patients for 15 years after treatment to study the effect of infusing virally-transduced vectors. I don't think that there's a clear answer as to whether the virus is an issue. You're also right, however, that it's necessary to test the stability of the transduced gene(s) , especially through passaging, holding and cryopreservation. All of this is nicely outlined here.