First of all, that is an excellent question! Secondly, please excuse the lack of thorough sourcing for this post. I only like to share some pointers...
Q: Can substances do more harm in a mammal at a lower dose than at higher dose?
A: Yes.
Some may know the example of the blood thinner, and widespread NSAID Acetyl-salicylic acid (Aspirin). I will use this example because Aspirin is one of the most known and used drugs in the world, with a long and interesting history. As being part of the class of nonsteroidal anti-inflammatory drugs (NSAIDs) it has recently gotten a bad wrap for blocking an enzyme which is crucial for prostaglandin synthesis and processes that maintain a healthy stomach wall in the presence of an potentially harmful bacterial and chemical milieu. On a sidenote, as an acid, Aspirin actually hardly dissolves directly in the acidic stomach.
To quote wikipedia (DOR: 28/09/2012):
Salicylates are excreted mainly by the kidneys as salicyluric acid
(75%), free salicylic acid (10%), salicylic phenol (10%), and acyl
glucuronides (5%), gentisic acid (< 1%), and 2,3-dihydroxybenzoic
acid.[148] When small doses (less than 250 mg in an adult) are
ingested, all pathways proceed by first-order kinetics, with an
elimination half-life of about 2.0 to 4.5 hours.[149][150] When higher
doses of salicylate are ingested (more than 4 g), the half-life
becomes much longer (15–30 hours),[151] because the biotransformation
pathways concerned with the formation of salicyluric acid and salicyl
phenolic glucuronide become saturated
Aspirin can interfere with a lot of drugs, including Ibuprofen. The known list of drugs is so high, in part due to the widespread application of aspirin, and in part due to the chemical composition of this very small drug with two functional groups. A functional group is a sort of chemical feature that determines how and with what probability a chemical interacts in a given milieu.
As a certain metabolic degradation pathway may get saturated, other pathways can take over and lead to different potentially harmful metabolites resulting in damage to the excretion/clearance organs such as the liver (hepatotoxic) and kidney (nephrotoxic).
A metabolite is the product of metabolism ( a weak back-referencing definition). metabolic pathways are a sequence of chemical reactions within a cell, and metabolism is the entire set of metabolites and pathways.
Liver/Kidney Toxicity is believed to result from an interplay of a) high concentrations of metabolites or direct toxins (=parent chemicals) within specialized high-concentration-forming cells, and b) the non/covalent binding of cellular macromolecules to interfere with their normal function and/or production of reactive oxygen species (ROS).
Another example (from memory) is the interaction pharmacokinetics of theobromine (from cacao) and other xanthines (unverified).
There are many more examples. I hope this example and mechanism serves you well as a starting point...
From a biochemical standpoint:
In fact drugs may act differently at different concentration thresholds at different times at different places within an organism and its cells that make it up. Evolution exploited this very early on and used it for things like body segmentation along defined axis during development.
Drugs may interact with each other differently at different levels of concentrations, say as binary, ternary, and higher order complexes. The rate of formation of such complexes is denoted through the dissociation constant - which is a type of equilibrium constant such as pH is.
The dissociation constant describes the propensity of a chemical species to separate reversibly and, - this is crucial! - is concentration dependent. This is accounted for by the use of so called activities or the apparent concentrations, as a result of incomplete hydration of the chemical and other effects of a "crowded environment". Now don't just think of chemicals, but macromolecules as well. In immunology for instance new molecular features can arise on the surface of a macromolecule, due to the association (complexation) with a small molecular drug. This in turn can lead to an immunological reaction, even anaphylaxis ( a so called Type I hypersensitivity reaction) and ultimately shock. Such drugs are classified as haptens.
Important in an organisms sensitivity and susceptibility to drugs however, is the current allometric growth rate and types of organs and cells available. As such a fetus is more susceptible than an adult.
I hope a simple yes accompanied by this admittedly to-long to really read post gave you some insight into what scientist across many, many fields are dealing with. Naturally, the issue is more complex.
Personally I believe the issue of dosing and drug reactions will improve significantly over the coming decade...
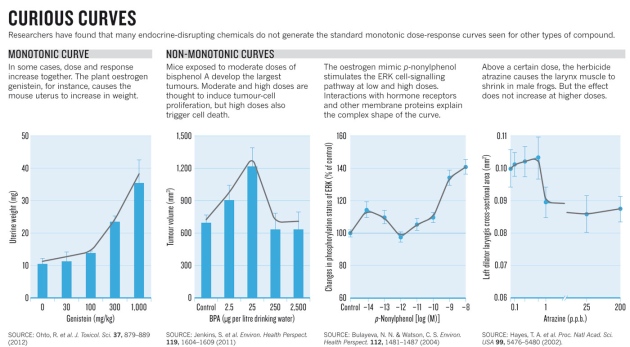 Nature is kind enough to allow access to this image. The three curves on the right show a decline in drug effect as concentration increases.
Nature is kind enough to allow access to this image. The three curves on the right show a decline in drug effect as concentration increases.