The question has a vague term cause which is confusing people here.
For me, it means that the event increases the risk of the outcome.
For some others, it means the event is a definite factor in resulting in the outcome.
So I avoid answering to the question Yes or No because of different interpretations of the term.
The systemic intravascular thombosis increases the risk of stroke, for example, through the two situations as described in Raoul's answer here but those are not sufficient for the accurate risk score of the stroke risk.
The factors of stroke risk interact with each other so we cannot leave this question just only about intravascular thombosis and stroke risk, but must consider stroke risk more generally.
CHA2VASc Score for General Stroke score
The Role of the Left Atrial Appendage in AF-Related Strokes, 2013.
Chads-Vasc score. CHA2 DS2-VASc.
SCORE
C CHF or LVEF < 40\% 1
H Hypertension 1
A Age > 75 2
D Diabetes 1
S Stroke/TIA/ HF
thromboembolism/ 2
V Vascular disease 1
A Age 65-74 1
S Sex Category female 1
Max points 9.
which specificity and sensitivity are not so high which has resulted in many variations of the initial CHAD VASc score, for example in this study:
We studied 94 patients, 66.0% male, mean age 64.4 years (standard
deviation 14.2). A cardioembolic source was detected in 20 patients.
ROC curve analysis identified as predictors of cardioembolic source
CHADS2 score ≥4 (sensitivity of 75.0%, specificity of 66.0%, p=0.014)
and CHA2DS2-VASc score ≥5 (sensitivity of 83.3%, specificity of 58.0%,
p=0.009).
To improve this score is ongoing research:
- CHADS2 as well as the CHA2DS2VASc risk score can exclude a large proportion of patients from having high risk of stroke or death, here
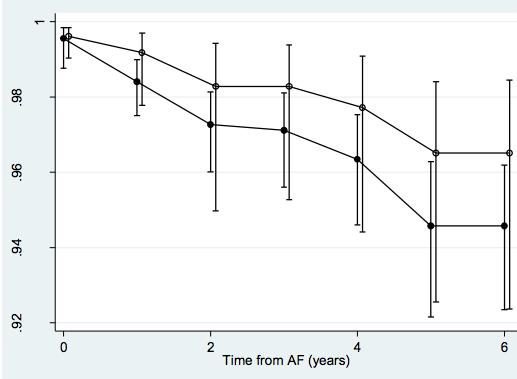
- Negative predictive value for zero as cut off value for the endpoint Stroke between CHADS2 (solid dots) and CHA2DS2VASc (circles) in Figure 1
Figure 1: CHADS2 (solid dots) and CHA2DS2VASc (circles).
Sources of thrombosis
- Atrial fibrillation and Left atrial appendix is the source where thrombus can spread into the great circulation
- Patent Foramen Ovale and Stroke where risk factors anatomic variation (PFO size, ASA, eustachian valve anatomy), hemodynamic parameters, presence of venous thrombus identified through higher-sensitivity tests such as lower extremity/abdominal/pelvic MRI, and the presence of hypercoagulable genetic variables
BBB's permeability and Stroke risk
The interaction of the permeability of the brain-blood barrier with the stroke risk is much unknown.
The following factors interact with the BBB's permeability
Cerebral Blood Flow (CBF) and stroke and Stroke Risk
CBF interaction with the risk of stroke is unknown field
- Alcohol effects on CBF in subjects with low and high responses to alcohol, here.
- carbonated water increases CBF
- aging decreases CBF (standard textbook MRI pictures)
Sources
- Stoll, Guido. Molecular mechanisms of thrombus formation in ischemic stroke: novel insights and targets for treatment. 2009. Online available.
- Homma, Shunichi, et al. Foramen Ovale and Stroke. 2005. Online available.
- Citings in the body of this question.