Physiology
My conjecture.
The slightly elevated position causes greater venous return (work against gravity by smooth musculature and thoracic pump).
Why this is happening this way is partially based on my question here about Fast standing and the heart's insufficient accommodation of the increased venous return.
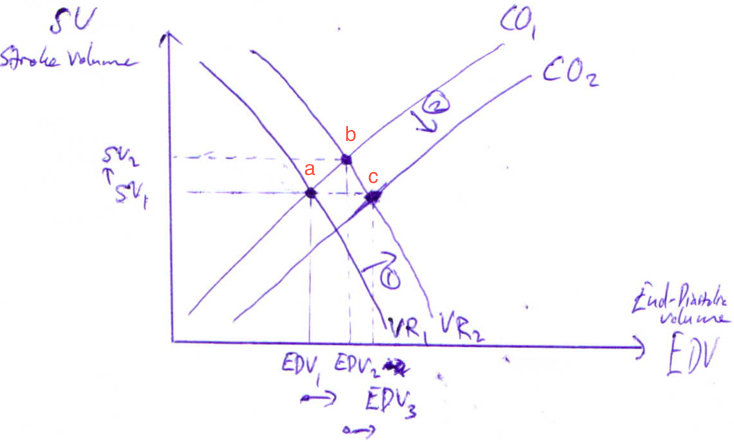
where the venous return reacts first the change in the position from supine by shifting the VR1 to VR2.
The stroke volume increases initially to SV1 to SV2, while the end diastolic volume from EDV1 to EDV2.
The increased stroke volume cannot be maintained long time so the cardiac output shifts to the right from CO1 to CO2.
So the initial stroke volume SV1 is the same as SV3 (not in the picture).
However, the EDV has increased (EDV3 >> EDV1) which increases much the lymphatic drainage.
Lymphatic drainage is not dependent on the stroke volume.
Increased lymphatic drainage then again increases the circulation of lymph.
This then again supports the recovery from the upper respiratory infection where the fine regulation between
- the thoracic pump,
- respiratory pump, and
- smooth musculature
determine the final effect of the body position on the recovery times.
The size of the thoracic cavity puts some limitations, for instance.
Cardiology
In some cases, the upper respiratory infection can cause myocarditis.
This will decrease the functioning of the heart and cause possible
- premature atrial contraction, and/or
- premature ventricular contraction.
Elevated position helps small arterioles of left ventricle supply preload.
Otherwise, ectopic beat can be heard or also called "epics beat" which is sign of the two previous conditions.
The nurse is educated to listen to the patient and ask for possible jolts and flips in the chest.
Elevating position in such a case can help because of better supply for preload in the left ventricle.
Pathophysiology
Upper respiratory infection is often acute respiratory infection (acute respiratory distress syndrome).
There is an increased permeability of the vessels.
The fluids and plasma proteins are going through alveoli.
Acute hyaline membranes are formed.
Cytokines play a big role in this process.
To maintain lymph retention, the result of increased venous return compensates.
These patients can breath normally in the sitting position.
There are also other reasons for the infection:
- overweight - the greater intra-abdominal pressure $\to$ more liquid diffused into the lungs OR other organs are suppressed.
- Big chest suppresses lungs such that the architecture can change.
Pharmacology
There are different drugs which effect is dependent on posture and position of the body.
Hypertension is a common disease which amount increases during ageing in population.
Let's take hypertensive drugs as a case study.
Peripherally acting sympathoplegic drugs are generally dependent on posture more than centrally acting ones.
In hypertension treatment, the peripheral acting sympatholegic drugs are used often in combination with diuretics.
Blood pressure can be under control when blood volume is 95% of normal, but much too high when blood volume is 105% of normal.
So this study should be considered with no hypertension and hypertension.
Sources
- For Pharmacology, Basic and Clinical Pharmacology, 11th edition, Katzung et all.