@Bryan's answer is good. I'd like to add a little structure around what seems to be the primary confusion in your question.
There are three important measurements here:
- $P_{aO_2}$
- $O_2$ saturation
- Hemoglobin concentration
$P_{aO_2}$
Arterial $P_{O2}$ ($P_{aO_2}$) is typically expressed in mm Hg. It is very specifically a measurement of the concentration of oxygen dissolved in arterial blood and NOT bound to hemoglobin. Low $P_{aO_2}$ is called hypoxemia.
$O_2$ saturation
$O_2$ saturation is a measurement of the percentage of Hemoglobin binding sites occupied by oxygen. It is expressed as a percentage, e.g., 98%.
Hemoglobin concentration
Hemoglobin concentration is a measurement of the concentration of hemoglobin protein in blood. It is typically expressed in the U.S. in g/dL.
Total oxygen content
Together, these three measurements ($P_{aO_2}$, $O_2$ saturation, and Hb concentration) determine the total oxygen content of arterial blood. Any one or any combination of these three measurements can result in hypoxia (inadequate oxygenation of tissue).
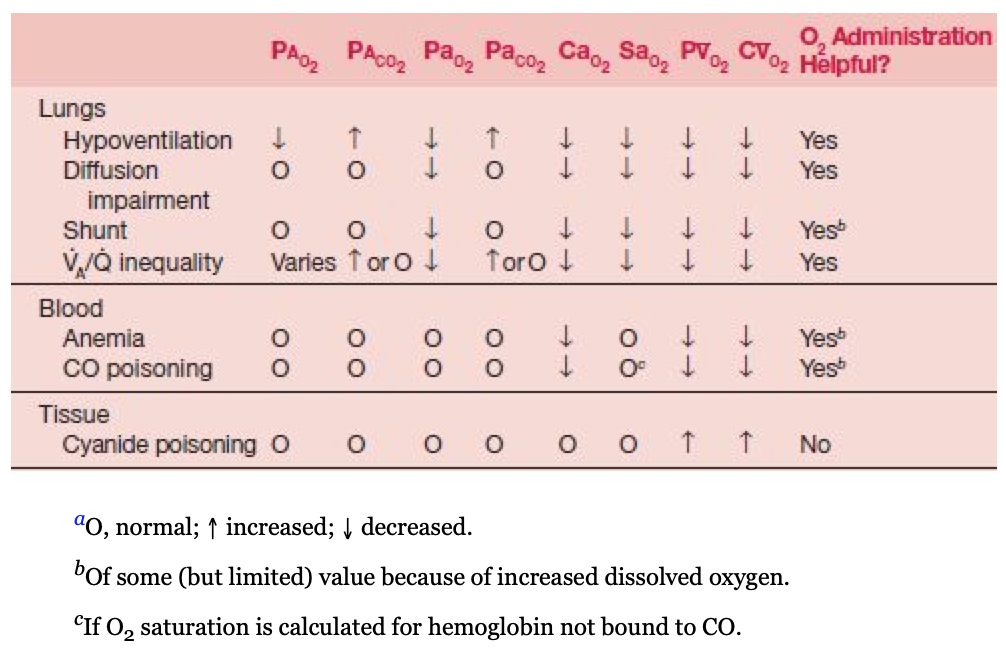
Carbon monoxide poisoning in an otherwise healthy individual is a specific cause of hypoxia that has a characteristic pattern: normal $P_{aO_2}$, normal Hemoglobin concentration, and low $O_2$ saturation. Because there is no problem breathing in oxygen or having it cross the blood gas barrier, there is a normal level of oxygen dissolved in arterial blood. $P_{aO_2}$ is normal. There is no anemia, so Hb concentration is normal. The problem is strictly a matter of $O_2$ saturation.
In many cases of hypoxia, the picture is mixed, but $CO$ poisoning is a classic example where the problem is exclusively one of $O_2$ binding. Anemia is another example. In anemia, $P_{aO_2}$ is normal, $O_2$ saturation is normal, but total oxygen content remains low because there is not enough Hemoglobin.
These are fairly complicated concepts, but covered quite well in West Respiratory Physiology, Ch. 6. The following table may be helpful. Note the footnote for $O_2$ saturation in the row for CO poisoning. Saturation is normal when calculated for Hemoglobin not bound to CO, in other words, there is nothing wrong with the Hb molecule itself. It is simply bound to something else. This is why administration of 100% $O_2$ is a useful treatment.